|
|
Necrotizing Fasciitis
General Considerations
- A rapidly progressive, infection of fascia which leads to subsequent necrosis of the subcutaneous tissue; muscles are frequently spared
- It may be caused by several organisms of groups of organisms
- Type 1: Polymicrobial
- Bacteroides, Clostridium, or Peptostreptococcus) in combination with streptococci other than group A and E. coli, Enterobacter, Klebsiella or Proteus
- Type 2: Group A beta-hemolytic streptococcus
- Clostridial infections (gas gangrene)
- Frequency may be increasing because of immunocompromised patients
- Organisms spread from subcutaneous tissue along both superficial and deep fascial planes
- Spread may be aided by bacterial enzymes and toxins.
- Carbon dioxide, hydrogen, nitrogen, hydrogen sulfide, and methane are produced from aerobic and anaerobic metabolism and lead to the presence of gas in the soft tissues
Clinical Findings
- Intense pain, sometimes out of proportion to the physical findings, and tenderness over involved area
- After a few days, nerve necrosis may produce anesthesia in the area, a clue to the presence of necrotizing fasciitis
- Edema, skin vesicular eruptions and crepitus
- Lymphangitis and lymphadenitis are infrequent
- Fever, malaise
- Surgical exploration is the only way to definitively establish the diagnosis of necrotizing infection and distinguish it from other entities
Imaging Findings
- Plain films are insensitive to the presence of gas in the soft tissues so that a negative conventional radiograph should not rule out the diagnosis
- Non-enhanced CT is the study of choice and may show thickening of fascial planes and gas in the subcutaneous tissue
- Gas is seen most often in Type 1 and that caused by Clostridium
- CT is specific but not highly sensitive
- In the absence of gas, surgical exploration is necessary
- MRI can be sensitive in determining the presence of necrosis and need for surgical debridement, combined with clinical evaluation
- Ultrasound may reveal subcutaneous collections of air and fluid not otherwise seen
Differential Diagnosis
Complications
- Of all patients with necrotizing fasciitis about 20-40% are diabetic
- May be seen in association with cardiac catheterization
- Vein sclerotherapy
- Diagnostic laparoscopy
- Possible association with non-steroidal anti-inflammatory drugs
- May be idiopathic, as in scrotal or penile necrotizing fasciitis (Fournier Gangrene)
Treatment
- Surgical emergency involving debridement of the affected areas
- Aggressive antibiotic therapy
- Hyperbaric oxygen treatment may be helpful
Prognosis
- Mortality rates from 20% to 80% have been reported
- Factors which affect prognosis include
- Pathogens
- Complicating diseases
- Infection site
- Rapidity with which treatment is instituted


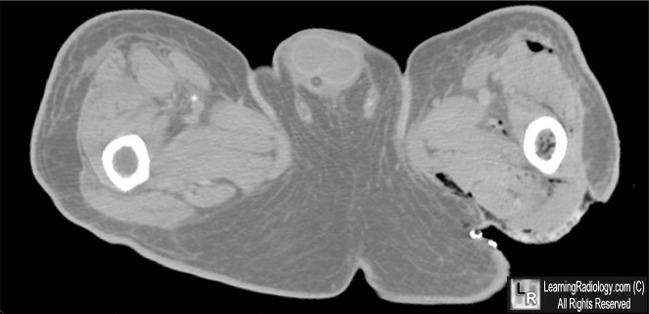
Necrotizing Fasciitis. Axial CT scans taken through the upper thighs show gas in the soft tissue fascial planes
(white circle and white arrows) in a patient with extreme tenderness in this region.
For this same photo without the arrows, click here and here
For more information, click on the link if you see this icon 
Necrotizing Fasciitis. eMedicine. Richard F Edlich
Necrotizing Soft Tissue Infections. Up-to-Date. Dennis L Stevens, and Larry M Baddou
|
|
|

{kind=link}
{kind=link}